Some of the common problems occurring at the Anus & Rectum
 |
Why suffer
in silence? |
SPECIALITY CENTRE FOR ANORECTAL PROBLEMS.
PILES (Haemorrhoids)
Piles ( Haemorrhoids )
Definition & Causes
Hemorrhoids, also spelled haemorrhoids, are vascular structures in the anal canal. In their normal state, they are cushions that help with stool control. They become a disease when swollen or inflamed; the unqualified term "hemorrhoid" is often used to mean the disease. The signs and symptoms of hemorrhoids depend on the type present. Internal hemorrhoids usually present with painless, bright red rectal bleeding when defecating. External hemorrhoids often result in pain and swelling in the area of the anus. If bleeding occurs it is usually darker. Symptoms frequently get better after a few days. A skin tag may remain after the healing of an external hemorrhoid.
While the exact cause of hemorrhoids remains unknown, a number of factors which increase pressure in the abdomen are believed to be involved. This may include constipation, diarrhea, and sitting on the toilet for a long time. Hemorrhoids are also more common during pregnancy. Diagnosis is made by looking at the area. Many people incorrectly refer to any symptom occurring around the anal area as "hemorrhoids" and serious causes of the symptoms should be ruled out.[2] Colonoscopy or sigmoidoscopy is reasonable to confirm the diagnosis and rule out more serious causes like rectal cancer.
Classification
Internal piles: Soft swellings of engorged, tortuous vessels, covered by mucus membrane inside the lower rectum, usually 3 in numbers.
External piles: Similar swellings outside the anal canal, below the anal skin.
Interno-external piles: Both the piles combined together.
Though the piles are present in every individual, unless they start giving trouble or become pathological, they should not be considered for the treatment.
HAEMORRHOIDS – ETIOLOGY
Causes: Hereditary- Morphological- Anatomical- Personal tendency to have piles.
Exciting causes: colitis, dysentery, diarrhea aggravates the latent hemorrhoids.
Secondary causes: straining due to constipation, carcinoma of rectum, pregnancy, urethral stricture or enlarged prostate.

Symptoms:
Bleeding: Slight to profuse. Prolapse : Piles comes out f of the anus as they grow. I to IV degree.
Mucous discharge: irritation & discomfort.
Pain: only if complications occur.
Anaemia: due to blood loss.
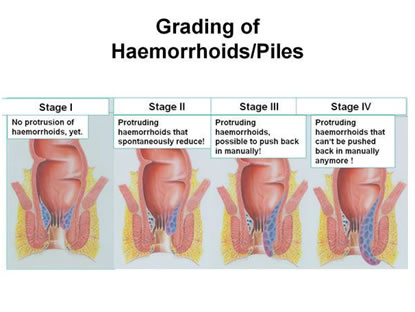
Stages of internal piles.
First degree Piles: Do not prolapse, but bleed. Seen through proctoscope.
Second Degree Piles: The piles comes out of the anus up to the anal verge but reverts back spontaneously if straining is over.
Third degree: The piles comes out of the anus & has to be pushed in digitally.
Fourth degree : The piles always remains outside the anus.
Complication of piles: Profuse bleeding, Inflammation, Ulceration, Thrombosis, Strangulation, Gangrene, Fibrosis, Suppuration & pyelephlebitis (rarely).
Treatment
Non operative or conservative treatment:
1) Antibiotics & other medicines, Hot water tub bath & Proprietary ointments- are given to reduce the infection, pain & swelling.
2) Laxatives to soften the stools.
3) Life style management of diet, rest & stool habits.
Non – operative Procedures
Rubber Band Ligation
By this method, mucosa ( containing the pile mass), 1-2 cms above the dentate line is grasped and pulled into a rubber band applier and a tight rubber band is applied at the base of the piles; cutting the blood supply of the haemorroid which eventually falls of and a scar is left at the site of band ligation. Rubber band ligation is mainly used for second degree piles.

Injection Sclerotherapy
1-3 ml of sclerosant agent ( 5 % phenol in almond oil or arachis oil, sodium morrhoate or sodium tetradecyl citrate ) is injected at the base of pile and into the substance of pile mass which causes thrombosis and sterile inflammation which eventually gets fibrosed and the pile mass is destructed. 1-3 injections at the interval of 4-7 days are required for satisfactory results. This is useful in the treatment of first, second & some cases of third degree piles to stop the bleeding. In some cases it could be curative but the recurrence is possible and eventually these cases may need surgery.

This can be performed as an office procedure and no admission is required. Since it is painless it does not require anaesthesia.
Infrared Photocoagulation
The infrared probe is applied to the base of haemorrhoids through a proctoscope to produce a circular burn 2 mm deep. Exposure is for 1 second at each site. Infrared Photocoagulation is an effective outpatient treatment for first and second degree haemorroids.
This is not a very popular method since it requires expensive instruments and the resultant ulceration may take long time to heal and cause discomfort to the patient for long time.
Surgical Procedures
Clamp and cautery hemorrhoidectomy
This method is now obsolete but has the advantage in not having any form of dissection of tissue planes. It used to cause severe post operative pain and stenosis of the anal canal, hence it is not in practice at present.
Open hemorrhoidectomy (Milligan-Morgan method)
This is the most commonly used technique and is widely practiced and effective surgical technique for treating hemorrhoids.
A V-shaped incision is made by the scalpel in the skin around the base of the hemorrhoid is followed by scissors dissection in the submucous space to strip the entire hemorrhoid from its bed. The dissection is carried cranially to the pedicle, which is ligated with strong catgut and the distal part excised. Other hemorrhoids are similarly treated, leaving a skin bridge in-between to avoid stenosis. The wound is left open and a hemostatic gauze pad left in the anal canal. The procedure is done under general or epidural anesthesia.
Postoperative pain and acute urine retention are common complications. Takes long time for healing and is not considered as an ideal procedure for the piles treatment.
Closed hemorrhoidectomy (Ferguson's technique)
Here the incisions are totally or partially closed with absorbable running suture, following surgical excision of the hemorrhoids . The Ferguson method has no advantage in terms of wound healing because of the high rate of suture breakage at bowel movement. There are several modifications of this method.
In this method there are marginal advantages of comparatively, having less pain and early healing because of primary closure of the wound and limited excision of the mucous membrane and of the anal skin.
Submucosal hemorrhoidectomy (Parks procedure)
It was designed to reduce postoperative pain and avoid anal and rectal stenosis. It is indicated for second- to fourth-degree hemorrhoids. A Parks retractor is inserted. A point just below the dentate line at the hemorrhoid is grasped with a hemostat. A 30-40–mL saline containing 1:400,000 parts adrenaline is injected submucosally to open up tissue planes and to reduce bleeding. Scissors are used to excise a small diamond of anal epithelium around the hemostat. The incision is continued cranially for 2.5 cm, creating two mucosal flaps on each side, which are each grasped with further hemostats, and submucosal dissection is commenced to remove the hemorrhoidal plexus from underlying internal sphincter muscle and overlying mucosa. This dissection is continued into the rectum, where the resulting broad base of tissue is suture-ligated and divided. The mucosal flaps are then allowed to flop back into position. No suture or any intra-anal dressing is used. Parks advocated use of suture for only prolapsed hemorrhoid to reconstitute the mucosal ligament,’ but most contemporary descriptions advocate suturing the mucosal flaps loosely together and to the underlying internal sphincter. The same procedure is carried out on the other hemorrhoids. Parks hemorrhoidectomy is done under general or epidural anesthesia. It is safe and associated with low rates of complications and recurrence. It however takes longer time and is more difficult to learn.
A recent study by Yang et al., 2005, concludes that the modified lift-up submucosal hemorrhoidectomy is an easier operative method compared with the procedure originally developed by Parks. However the external haemorroids and skin tags are not taken care of in this procedure.
Pile ‘suture’ method
Also called the pile stitching method, it was first described in 1978 by Faraq for hemorrhoids of grades II and III. The method entails use of three interrupted sutures to secure the hemorrhoids in place without excision.
Can be used only for internal haemorrhoids and high incidences of recurrence is the major issue.
Advanced Techniques
LASER hemorrhoidectomy
The hemorrhoid is vaporized or excised using carbon dioxide or NdYag LASER. The smaller LASER beam allows for precision and accuracy; and, usually, rapid, unimpaired healing. It is painless. LASER therapy may be used alone or in combination with other modalities.
Laser is a cutting tool with advantage of precision cutting and minimal lateral dissemination of energy. Hence it causes minimal tissue damage and the healing is faster. However the laser cannot be effective in presence of liquids like blood and has a limitation in the treatment of piles. It has a marginal advantage of having less pain and early healing of the internal piles but if used for the external piles there is no advantage over the other methods.
Radiofrequency ablation and suture fixation of hemorrhoids
It is an innovative procedure for hemorrhoids of grades III and IV. The procedure entails the use of an Ellman dual-frequency, 4-MHz radiofrequency generator for ablation of hemorrhoids. Radiofrequency waves ablate tissue by converting radio waves into heat. The alternating current generates changes in the direction of ions within the tissue fluid. This creates ionic agitation and frictional heating, leading to coagulative necrosis of tissue. Thereafter, the hemorrhoids are plicated using strong absorbable sutures. The plication begins from the most distal end of the hemorrhoid at the anal verge and is carried towards the pedicle in a continuous locking manner and knotted at the pedicle, thereby fixing the hemorrhoidal mass. It gives better results in terms of postoperative pain and bleeding than stapled hemorrhoidectomy and Doppler-guided hemorrhoidal artery ligation.
Bipolar diathermy hemorrhoidectomy
This operation is indicated mostly for second- to fourth-degree hemorrhoids. With the aid of a bipolar diathermy set on cutting and coagulation, dissection is carried from a V-shaped incision in the skin around the base of the hemorrhoid unto the pedicle, which is dissected and divided .The diathermy is set on coagulation only during dissection and division of the pedicle. No ligature is used. A randomized trial study by Andrews et al. showed that diathermy hemorrhoidectomy has no significant advantage as far as post operative pain and healing is concerned.
Ligasure and Starion hemorrhoidectomy with submucosal dissection
The ligasure vessel-sealing generator is an isolated-output electrosurgical generator that provides power for vessel sealing and bipolar surgery. It provides precise thermal energy delivery and electrode pressure to vessels to achieve complete and permanent fusion of the vessel lumen. The Starion thermal welding system is similar to the ligasure generator but uses the tissue-welding technology to simultaneously fuse vessels and tissue structures closed. The operating temperature is less than 100°C, thereby producing less heat and collateral tissue damage. The operation is done under general or epidural anesthesia. A V-shaped incision at the junction of the hemorrhoid and the peri-anal skin is made by a scalpel, followed by dissection of the hemorrhoidal bundles off the underlying sphincter. The ligasure or Starion handset is applied to the dissected hemorrhoids and activated to seal mucosal edges and divide the pedicle. A hemostatic sponge is inserted into the anal canal. Wang et al. demonstrated that the Starion hemorrhoidectomy has marginally less postoperative pain and parenteral analgesic requirement than ligasure hemorrhoidectomy, but both have the same advantages of shorter operating time and less blood loss but overall healing process remains the same compared to the other conventional methods.
Harmonic Haemorrhoidectomy
Recently ultrasonic energy being used for the tissue cutting has been tried for the piles surgery. This has advantage of precise cutting, less thermal damage and limited lateral dissemination of energy. The benefits are less bleeding, marginally less pain, however the healing process remains the same as other methods.
Stapled hemorrhoidectomy
This procedure is also known as circumferential mucosectomy or ‘procedure for prolapse and hemorrhoids’ (PPH). It was first described in 1998 by Longo for prolapsing second- to fourth-degree hemorrhoids. He suggested that stapled resection of a complete circular strip of mucosa above the dentate line lifts the hemorrhoidal cushions into the anal canal. In PPH, the prolapsed tissue is pulled into a circular stapler that allows the excess tissue to be removed while the remaining hemorrhoidal tissue is stapled. A circular anal dilator is introduced into the anal canal. The prolapsed mucous membrane falls into the lumen after removing the dilator. A purse-string suture anoscope is then introduced through the dilator, to make a submucosal purse-string suture around the entire anal canal circumference. The circular stapler is opened to its maximum position. Its head is introduced and positioned proximal to the purse-string suture, which is then tied with a closing knot .The entire casing of the stapler is then pushed into the anal canal, tightened and fired to staple the prolapse. Firing the stapler releases a double-staggered row of titanium staples through the tissue. A circular knife excises the redundant tissue, thereby removing a circumferential column of mucosa from the upper anal canal. The staple line is then examined with the anoscope for bleeding, which if present may be controlled by placement of absorbable sutures. The staple line should be maintained at a distance of 3-3.5 cm from the anal verge to avoid postoperative rectal stenosis and pain. Patients experience less pain and achieve a quicker return to work compared to conventional procedures; and bleeding is less.

Requires a costly specialized single use instrument. This procedure has a high learning curve. There is no excision or destruction of the heamorroidal mass, hence the chances of recurrence always remains. At the same time in this procedure large external piles are not addressed and excision of the external piles looses the advantage of having less pain post operatively. Bleeding, retention of urine, rectal stenosis remains the other complications post operatively. The patient selection is most important and hence cannot be called as a Gold Standard for all types of haemorrhoids.
Doppler-guided hemorrhoidal artery ligation
This is also a new technique in which the hemorrhoidal arteries are identified by means of a Doppler (ultrasound) technique.The specially designed proctoscope contained a Doppler transducer and a window through which the surgeon can identify and ligate the hemorrhoidal arteries by placing a suture around them. All the hemorrhoidal arteries are ligated in this procedure. It is a day care procedure suitable for first-, second- and some selected third-degree hemorrhoids, and the patient goes home after sedation wears off. There is little or no bleeding postoperatively. Pure external hemorrhoids would not respond to this procedure.
This procedure is advantageous as far as bleeding is concerned. However the post operative pain, discomfort & duration of recovery makes marginal difference than with other methods.

Atomizing hemorrhoids
The atomizer wand is an innovative wave form of electrical current wherein a specialized electrical probe excises or vaporizes one or more cell layers at a time, reducing the hemorrhoids to minute particles of fine mist or spray, which are immediately vacuumed away. The hemorrhoids are essentially disintegrated into an aerosol of carbon and water molecules. Results are similar to those of LASER hemorrhoidectomy except that there is less bleeding using the atomizer and that the atomizer costs less. The procedure is suitable for hemorrhoids of grades I, II and III. Patient does not require hospital stay. Presently, atomizing hemorrhoids is offered exclusively in Arizona, USA.
Special Consideration / Complicated Piles
Acutely thrombosed or strangulated internal hemorrhoids
Patients with acutely thrombosed or strangulated internal hemorrhoids usually present with severely painful and irreducible hemorrhoids. The incarcerated hemorrhoids may become necrotic and drain. This situation is quite difficult to treat particularly in a case of extensive strangulation or thrombosis or the presence of underlying circumferential prolapse of high-graded hemorrhoids. Manual reduction of the hemorrhoid masses, with or without intravenous analgesia or sedation, might help reducing pain and tissue congestion. Urgent hemorrhoidectomy is usually required in these circumstances. Unless the tissues are necrotic, mucosa and anoderm should be preserved as much as possible to prevent postoperative anal stricture. In expert hands, surgical outcomes of urgent hemorrhoidectomy were comparable to those of elective hemorrhoidectomy.
Acutely thrombosed external hemorrhoids
Acutely thrombosed external hemorrhoids often develop in patients with acute constipation, or those with a recent history of prolonged straining. A painful bluish-colored lump at the anal verge is a paramount finding. The severity of pain is most intense within the first 24-48 h of onset. After that, the thrombosis will be gradually absorbed and patients will experience less pain. As a result, surgical removal of acute thrombus or excisional hemorrhoidectomy may be offered if patients experience severe pain especially within the first 48 h of onset. Otherwise, conservative measure will be exercised including pain control, warm sitz baths, and avoidance of constipation or straining. A resolving thrombosed external hemorrhoid could leave behind as a residual perianal skin tag -which may or may not require a subsequent excision.
Hemorrhoids in pregnancy
Hemorrhoids are very common during pregnancy especially in the third trimester. Acute crisis such as profound bleeding and irreducible prolapsing may be found in pregnant women with pre-existing hemorrhoids. Since hemorrhoids and its symptoms will gradually resolve after giving birth, the primary goal of treatment is to relief acute symptoms related to hemorrhoids - mostly by means of dietary and lifestyle modification. Kegel exercises, lying on left side, and avoidance of constipation could reduce the episode and severity of bleeding and prolapse. Fiber supplement, stool softener and mild laxatives are generally safe for pregnant women. Topical medication or oral phlebotonics may be used with special caution because the strong evidence of their safety and efficacy in pregnancy is lacking. In case of massive bleeding, anal packing could be a simple and useful maneuver. Hemorrhoidectomy is reserved in strangulated or extensively thrombosed hemorrhoids, and hemorrhoids with intractable bleeding.
Hemorrhoids in immunocompromised patients
In general any intervention or operation should be avoided, or performed with a careful consideration in immunocompromised patients because of an increases risk of anorectal sepsis and poor tissue healing in such cases. A conservative measure is the mainstay for the treatment of hemorrhoids in this group of patients. If required, injection sclerotherapy appeared to be a better and safer alternative to banding and hemorrhoidectomy for treating bleeding hemorrhoids. Antibiotic prophylaxis is always given before performing any intervention, even a minor office-based procedure, due to the possibility of bacteremia.
Often patients are suffering from opportunistic infections which needs to be treated simultaneously. At the same time usually the piles are infected and severe anal spasm adds to the discomfort and pain. Antibiotic therapy, Sitz bath ( sitting in hot water ) and regular dilation with the help of anal dilators keeps the patient comfortable.
Hemorrhoids in patients having anticoagulant or antiplatelet drugs
Anticoagulant or antiplatelet drugs may promote anorectal bleeding in patients with hemorrhoids and increase risk of bleeding after banding or surgery. Unless the bleeding is persistent or profound, the discontinuity of antithrombotic drugs may be unnecessary because most of the bleeding episodes are self-limited and stop spontaneously. Conservative measure is therefore the mainstay treatment in these patients. Injection sclerotherapy is a preferential treatment for bleeding low-graded hemorrhoids refractory to medical treatment. Rubber band ligation is not recommended in patients with the current use of anticoagulant or antiplatelet drugs due to the risk of secondary bleeding. If banding or any form of surgery for hemorrhoids is scheduled, the cessation of anticoagulant or antiplatelet drugs about 5-7 d before and after the procedure is suggested
Comments:
As the exact pathophysiology of haemmorhoids is not understood till now. The ideal treatment for the cure of piles is not developed as yet. The different methods advised for various degrees of piles are not 100% satisfactory and pain, bleeding and recurrence remains the main issues with different modalities of treatment. No method of treatment can be described as a Gold Standard for the treatment of all degrees and varities of piles. Of the prevailing modalities of the treatment for first and second degree piles, sclerotherapy and banding being the most popular methods of treatment, however sclerotherapy has high rate of recurrence and banding may be very painful at times. Among the conventional methods of surgery the principle remains that of excision of pile mass and closure of the wound to allow it to heal by secondary intention. Bleeding, post operative pain, long recovery period, stenosis and recurrence are the side effects of the procedure.
Of the newer methods of treatment most of the methods described destruction of the pile mass with different energy sources. There is hardly any difference in post operative pain and recovery period.
The staple haemoroidectomy has an advantage in second and third degree piles of having less pain and early recovery. But the recurrence rate is very high. It requires a costly instrument and the learning curve is also very high. Thus staple haemoroidectomy has a disadvantage of not addressing the external piles. If the external piles are to be excised the advantage of having less pain and early recovery is nullified.
THD has again the disadvantage of requiring a specialized machine and significant post operative pain along with chances of recurrence.
In every individual there could be a different presentation of piles, each pile having different degree and hence the treatment has to be individualized. The very fact that number of procedure are being describes for the treatment of piles yet no procedure is fully satisfactory. The search for newer techniques will continue till all the criteria of piles treatment are satisfied fully.
It has been observed that in some of the patients even if the piles are small ,i.e., first or second degree, they bleed profusely, the blood is bright red color and the patient may become anemic very fast and may require blood transfusion for the recovery. Most of the piles bleed chronically over a long period with exacerbation and remission without necessiting the blood transfusion. Though not mentioned in the literature, it appears that in a small subset of patients the piles are predominantly arterial in nature and which can be seen pulsating on the operation table. These piles are likely to bleed profusely even if they are small, i.e. first to second degree and surgery would be recommended for theses piles even in early stages. Most of the patient would be having venous predominance and these piles will progress gradually
FUTURE PERSPECTIVES IN THE TREATMENT OF HEMORRHOIDS
The combinations of vasoconstrictive and venoconstrictive agents, with or without anti-inflammatory drugs, might be a new pharmacological approach for hemorrhoids.
Despite advances in office-based procedures and better surgical approaches, post-procedural pain and disease recurrence remain the most challenging problems in the treatment of hemorrhoids. Consequently, future researches and novel management of hemorrhoids may focus on how to minimize pain following a procedure and how to prevent recurrent hemorrhoids. Meanwhile, long-term results of newly or recently developed interventions are definitely required.
In conclusion, the better understanding of the pathophysiology of hemorrhoids would prompt the development of effective treatments for hemorrhoids. Preventive measures, by means of dietary and lifestyle modification, may be the best treatment of hemorrhoids. Once hemorrhoids develop, its treatment options mainly depend on the type and severity of hemorrhoids, patient’s preference and the expertise of physicians. Post-procedural pain and disease recurrence remain the most challenging problems in the treatment of hemorrhoids.