Some of the common problems occurring at the Anus & Rectum
 |
Why suffer
in silence? |
SPECIALITY CENTRE FOR ANORECTAL PROBLEMS.
Colorectal Cancer: Causes, Symptoms and Treatments
Colorectal cancer, also known as bowel cancer, colon cancer or rectal cancer, is any cancer (a growth, lump, tumor) of the colon and the rectum. The World Health Organization and CDC say it is the second most common cancer worldwide, after lung cancer
The American Cancer Society suggests that about 1 in 20 people in the US will develop colorectal cancer during their lifetime, with the risk being slightly higher for men than for women. Due to advances in screening techniques and improvements in treatments, the death rate from colorectal cancer has been dropping for over 20 years.
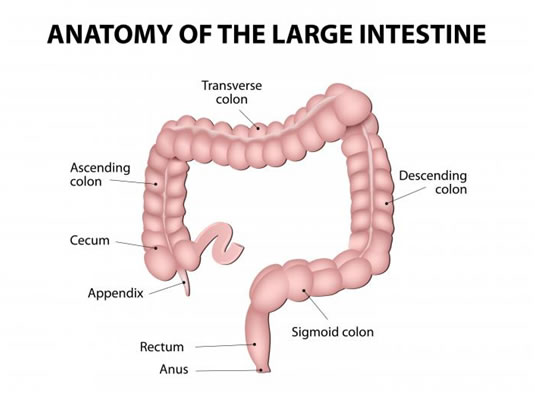
large intestine is also called the colon or large bowel.
The colon and rectum belong to our body's digestive system - together they are also known as the large bowel.
The colon reabsorbs large quantities of water and nutrients from undigested food products as they pass along it.
The rectum is at the end of the colon and stores feces (stools, waste material) before being expelled from the body.
Symptoms of colorectal cancer:
? Going to the toilet more often.
? Diarrhea.
? Constipation.
? A feeling that the bowel does not empty properly after a bowel movement.
? Blood in feces (stools).
? Pains in the abdomen.
? Bloating in the abdomen.
? A feeling of fullness in the abdomen (maybe even after not eating for a while).
? Vomiting. ? Fatigue (tiredness).
? Inexplicable weight loss.
? A lump in the tummy or a lump in the back passage felt by your doctor.
? Unexplained iron deficiency in men, or in women after the menopause.
As most of these symptoms may also indicate other possible conditions, it is important that the patient sees a doctor for a proper diagnosis. Anybody who experiences some of these symptoms for four weeks should see their doctor.
Causes of colorectal cancer:
Experts say we are not completely sure why colorectal cancer develops in some people and not in others. However, several risk factors have been identified over the years - a risk factor is something which may increase a person's chances of developing a disease or condition.
The possible risk factors for colorectal factors are:
? Being elderly - the older you are the higher the risk is.
? A diet that is very high in animal protein.
? A diet that is very high in saturated fats.
? A diet that is very low in dietary fiber.
? A diet that is very high in calories.
? A diet that is very high in alcohol consumption.
? Women who have had breast, ovary and uterus cancers.
? A family history of colorectal cancer.
? Patients with ulcerative colitis.
? Being overweight/obese.
? Smoking. This study found that smoking is significantly associated with an increased risk for colorectal cancer and death.
? Being physically inactive.
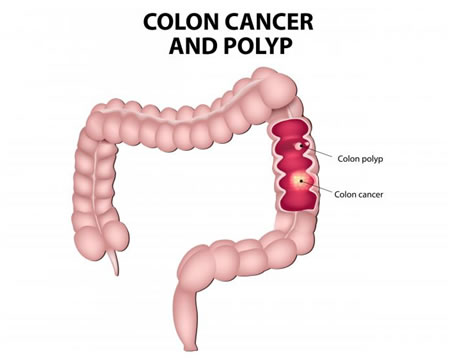
? Presence of polyps in the colon/rectum. Untreated polyps may eventually become cancerous.
? Having Crohn's disease or Irritable Bowel Disease have a higher risk of developing colorectal cancer.
Most colon cancers develop within polyps (adenoma). These are often found inside the bowel wall.
Recent developments on colorectal cancer causes from MNT news :
Being very overweight or obese in late teens may raise later-life colorectal cancer risk
Men who are very overweight or obese during late adolescence may be more than twice as likely to develop colorectal cancer by middle age. This is according to a new study published in Gut - a journal of The BMJ.
Eating processed meats can cause colorectal cancer, WHO
Eating processed meats can cause colorectal cancer, concludes a new report from the World Health Organization, while eating red meats may also raise risk for the disease.
Tumor suppressor gene promotes some colorectal cancers
Sprouty2, a gene known to stop tumors spreading to other parts of the body in many types of cancer, appears to play the opposite role in some forms of colorectal cancer. This was the finding of a study published in the journal Oncogene and led by the University of Missouri School of Medicine in Columbia, which may spur new treatments for colorectal cancer.
How obesity promotes colorectal cancer
Scientists have revealed a biological connection between obesity and colorectal cancer, and they have identified an approved drug that might prevent the cancer from developing. The findings are published in Cancer Research.
How common is colorectal cancer?:
According to WHO (World Health Organization) colorectal cancer is the second most common tumor among both men and women (after lung tumors).
Approximately 2% of over 50-year-olds will eventually develop colorectal cancer in Western Europe.
40% of people who are diagnosed with colorectal cancer are already at an advanced stage of the cancer. For these patients surgery is probably the most likely option.
Colorectal cancer tends to affect men and women equally. However, men tend to develop it at a younger age.
Tests and Diagnosis for colorectal cancer
Screening can detect polyps before they become cancerous, as well as detecting colon cancer during its early stages when the chances of a cure are much higher. The following are the most common screening and diagnostic procedures for colorectal cancer:
Fecal occult blood test (blood stool test)
This checks a sample of the patient's stool (feces) for the presence of blood. This can be done at the GP's (general practitioner's, primary care physician's) office. However, most patients are given a kit that explains how to take the sample at home. The patient then returns the sample to the doctor's office, and it is sent to a laboratory.
A blood stool test is not 100% accurate - it might not detect all cancers because not all of them bleed. Even cancers that do bleed often do not do so all the time. Therefore, it is possible that a patient has a negative result, even though he/she has cancer. Even if blood is detected, this may be caused by other illnesses or conditions, such as hemorrhoids. Some foods may suggest blood in the colon, when in fact, none was present.
Stool DNA test
This test analyzes several DNA markers that colon cancers or precancerous polyps cells shed into the stool. Patients may be given a kit with instructions on how to collect a stool sample at home. This has to be brought back to the doctor's office, and is then sent to a laboratory.
This test is much more accurate for detecting colon cancer than polyps. However, it cannot detect all DNA mutations which may indicate that a tumor is present.
Flexible sigmoidoscopy
The doctor uses a sigmoidoscope, a flexible, slender and lighted tube, to examine the patient's rectum and sigmoid (the sigmoid colon is the last of the colon, before the rectum). The test does not generally take more than a few minutes and is not painful; but might be uncomfortable. There is a small risk of perforation of the colon wall. If the doctor detects a polyps or colon cancer he/she will then carry on a colonoscopy to examine the entire colon and take out any polyps that are present - they will then be examined under a microscope.
A sigmoidoscopy will only detect polyps or cancer present at the end third of the colon and the rectum. If there are any in any other parts of the digestive tract it will not detect them.
Barium enema X-ray
Barium is a contrast dye that is placed into the patient's bowel in an enema form - it shows up on an X-ray. In a double-contrast barium enema air is added as well. The barium fills and coats the lining of the bowel, creating a clear image of the rectum, colon, and occasionally of a small part of the patient's small intestine. This procedure is often carried out along with a flexible sigmoidoscopy to detect any small polyps the barium enema X-ray may have missed. If the barium enema X-ray detects anything abnormal, the doctor may recommend a colonoscopy.
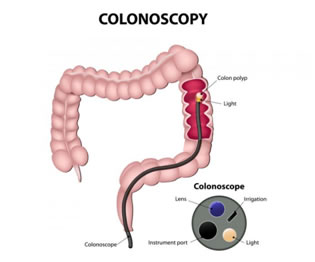
The doctor uses a colonoscope, which is much longer than a sigmoidoscope. A colonoscope is a long, flexible and slender tube which is attached to a video camera and monitor. The doctor can see the whole of the colon and rectum. Any polyps discovered during this exam can be removed there and then - sometimes tissue samples (biopsies) may be taken instead. Taking biopsies does not hurt.
Although colonoscopies are painless, some patients are given a mild sedative to calm them down. Prior to the exam the patient may be given a large amount of laxative fluid to clean out the colon (enemas are rarely used). Bleeding and perforation of the colon wall are possible complications, but extremely rare.
CT colonography (virtual colonoscopy)
A CT (computerized tomography) machine is used to take images of the colon. The patient needs to have a cleared colon for this exam to be effective. Even if anything abnormal is detected, the patient will then need conventional colonoscopy. A study found that CT colonography may offer patients at increased risk of colorectal cancer an alternative to colonoscopy that is less-invasive, is better-tolerated and has good diagnostic accuracy.
Ultrasound scan
Sound waves are used to help show if the cancer has spread to another part of the body.
Magnetic resonance imaging (MRI)
This gives a three-dimensional image of the bowel and may help the doctor in his/her diagnosis.
PET SCAN Positron-emission tomography (PET)[1] is a nuclear medicine functional imaging technique that is used to observe metabolic processes in the body. The system detects pairs of gamma rays emitted indirectly by a positron-emitting radionuclide (tracer), which is introduced into the body on a biologically active molecule. Three-dimensional images of tracer concentration within the body are then constructed by computer analysis. In modern PET-CT scanners, three-dimensional imaging is often accomplished with the aid of a CT X-ray scan performed on the patient during the same session, in the same machine.
If the biologically active molecule chosen for PET is fludeoxyglucose (FDG), an analogue of glucose, the concentrations of tracer imaged will indicate tissue metabolic activity as it corresponds to the regional glucose uptake. Use of this tracer to explore the possibility of cancermetastasis (i.e., spreading to other sites) is the most common type of PET scan in standard medical care (90% of current scans). However, although on a minority basis, many other radioactive tracers are used in PET to image the tissue concentration of other types of molecules of interest. One of the disadvantages of PET scanners is their operating cost.[2]
In cancer PET scan is recommended
- To detect the cancer.
- To know the spread & staging of the cancer.
- To detect recurrence of the cancer.
- To assess the effect of the treatment.
- To detect Hidden (Occult) cancers.
Staging the cancer
The stage of a cancer means the extent of the cancer. As soon as a colon cancer diagnosis has been made the doctor will determine its stage - this helps chose the most appropriate treatment. The stages of colon cancer are:
- Stage 0 (Also known as Duke A stage). - the earliest stage. It is still within the mucosa (inner layer) of the colon or rectum - also called carcinoma in situ.
- Stage I (Also known as Duke B stage). - it has grown through the inner layer of the colon or rectum, but has not yet spread beyond the wall of the rectum or colon.
- Stage II (Also known as Duke C stage). - it has grown through or into the wall of the colon or rectum. However, it has not reached the nearby lymph nodes yet.
- Stage III (Also known as Duke D stage). - the nearby lymph nodes have been invaded by the cancer, but it has not yet affected other parts of the body.
- Stage IV (Also known as Duke E stage). - it has spread to other parts of the body, including other organs, such as the liver, the membrane lining the abdominal cavity, lung, or ovary.
Recurrent - the cancer has returned after treatment. It may come back and affect the rectum, colon, or elsewhere in the body. Scientists have found that the presence of a biomarker in regional lymph nodes is an independent predictor of disease recurrence in patients with colorectal cancer.

Treatments for colorectal cancer
The patient's treatment will depend on several factors, including its size and location, the stage of the cancer, whether or not it is recurrent, and the current overall state of health of the patient. A good specialist will explain all the treatment options available to the patient. This is an opportunity for the patient to ask questions and get advice on lifestyle changes that will help recovery. Treatment options include chemotherapy, radiotherapy, and surgery:
Surgery for colorectal cancer
This is the most common colorectal cancer treatment. The affected malignant tumors and any lymph nodes that are nearby will be removed. Surgeons remove lymph nodes because they are the first place cancers tend to spread to.
The bowel is usually sewn back together. On some occasions the rectum may need to be taken out completely - a colostomy bag is then attached for drainage. The colostomy bag collects stools and is generally placed temporarily - sometimes it may be a permanent measure if it is not possible to join up the ends of the bowel.
If the cancer is diagnosed early enough, surgery may be the only treatment necessary to cure the patient of colorectal cancer. Even if surgery does not cure the patient, it will ease the symptoms.
Chemotherapy
Chemotherapy involves using a medicine (chemical) to destroy the cancerous cells. It is commonly used for colon cancer treatment. It may be used before surgery in an attempt to shrink the tumor. A study found that patients with advanced colon cancer who receive chemotherapy and who have a family history of colorectal cancer have a significantly lower likelihood of cancer recurrence and death.
Radiotherapy
Radiotherapy uses high energy radiation beams to destroy the cancer cells, and also to prevent them from multiplying. This treatment is more commonly used for rectal cancer treatment. It may be used before surgery in an attempt to shrink the tumor.
Doctors may order both radiotherapy and chemotherapy after surgery as they can help lower the chances of recurrence.
Recent developments on colorectal cancer prevention and treatment from MNT news
Aspirin, NSAIDs linked to reduced risk of colorectal cancer
Risk from colorectal cancer could be reduced through the long-term use of low-dose aspirin and non-aspirin nonsteroidal anti-inflammatory drugs, a new study published in the Annals of Internal Medicine shows.
How can aspirin help to cure cancer?
A recent study, published in the journal Cell, suggests that aspirin could be effective in boosting the immune system in patients suffering from breast, skin and bowel cancer.
Gene may predict recurrence of bowel cancer A gene linked to bowel cancer recurrence and shortened survival could help predict outcomes for patients with the gene - and take scientists a step closer to development of personalized treatments, reveals research in the journal Gut.
300 oranges' worth of vitamin C impairs cancer cells
The power of vitamin C could one day be harnessed to fight colorectal cancer, according to a new study published in Science.
Daily coffee, even decaf, may protect against colorectal cancer
Researchers from the US and Israel found that drinking coffee every day - even decaffeinated coffee - may lower the risk of colorectal cancer.
Recovery from colorectal cancer
Malignant tumors will most probably grow and spread to other parts of the body if left untreated. The chances of a complete cure depend enormously on how early the cancer is diagnosed and treated. A patient's recovery depends of the following factors:
? The cancer stage when diagnosis was made.
? Whether a hole or blockage was created in the colon by the cancer.
? Whether the cancer has come back.
? The patient's general state of health.
Prevention of colorectal cancer
We can do quite a lot to lower our chances of developing colorectal cancer:
? Regular screenings - especially if you have had colorectal cancer before, you are over 60, there is a family history of this type of cancer, you have Crohn's disease. Some experts say screening should start after the age of 50.
? Nutrition - make sure your diet has plenty of fiber, fruit, vegetables, and good quality carbohydrates. Keep your consumption of red meat and processed meat down to a minimum, or cut them out altogether. Switch from saturated fats to good quality fats, such as avocado, olive oil, fish oils, and nuts. However, this study found that although vegetarians have an overall lower risk of developing cancers, their risk of developing colorectal cancer is higher than meat eaters.
? Exercise - exercise regularly. Moderate, regular exercise has been shown to have a significant impact on lowering a person's risk of developing colorectal cancer.
? Bodyweight - keep your bodyweight healthy. Being overweight or obese raises a person's risk of developing many cancers, including colorectal cancer.
Surgery for Rectal Cancer
COLORECTAL CANCER FACT SHEET
Colorectal cancer is the second-leading cancer killer of men and women combined in the U.S. More than 90 percent of colorectal cancer cases are discovered in people age 50 and over.
Overview
Surgery is a common treatment for rectal cancer. The type of operation used to remove the rectal cancer depends on the extent and location of the cancer. If the rectal cancer is located well above the anus, a low anterior resection (LAR) can be performed. This operation allows the patient to keep anal function and pass stools in a normal manner. If the rectal cancer is located close to the anus, sometimes the anus must be removed with the cancer in an operation called an abdominoperineal resection (APR). The patient must then use a colostomy bag. A colostomy is an opening where the large intestine is attached to the abdominal wall. A replaceable bag that encloses the colostomy is worn by the patient to collect stool.
Low Anterior Resection Surgery (LAR)
LAR is a common treatment for rectal cancer when the cancer is located well above the anus. During a LAR, the entire rectal cancer, adjacent normal rectal tissue and surrounding lymph nodes are removed through an incision made in the lower abdomen. After the cancer is removed, the cut ends of the rectum are sewn back together. The passage of stool from the large intestine through the anus is therefore preserved. If the cancer is lower in the rectum, the cut end of the large bowel may be attached directly to the anus, a procedure known as colo-anal anastomosis. When a colo-anal anastomosis is performed, some surgeons will create a temporary colostomy in order to protect the delicate surgical connection of the large intestine to the anus. After the patient has recovered from the surgery, the temporary colostomy is removed and stool is again passed normally through the large intestine. The colon is resewn to the anus.
Despite undergoing complete surgical removal of rectal cancer, some patients may experience recurrence of their cancer. It is important to realize that some patients with rectal cancer already have small amounts of cancer that have spread outside the rectum and were not removed by surgery. These cancer cells are referred to as micrometastases and cannot be detected with any of the currently available tests. The presence of these microscopic areas of cancer causes the relapses that follow treatment with surgery alone. External beam radiation therapy and chemotherapy can be used to cleanse the body of micrometastases in order to improve the cure rate achieved with surgical removal of the cancer.
Patients undergoing an LAR may experience lower abdominal pain after the operation. Less common complications related to surgery include bleeding, infection and temporary difficulty with emptying the bladder. Some men may experience sexual dysfunction after surgery. In-hospital death occurs after LAR in less than 5% of patients. Patients should ask their surgeon to explain the various surgical complications and their frequency of occurrence at the hospital where the surgery will be performed.
Abdominoperineal Resection Surgery (APR)
APR is a common treatment for rectal cancer when the cancer is located close to the anus. During an APR, the entire rectal cancer, adjacent normal rectum, rectal sphincter or anus, and surrounding lymph nodes are removed through an incision in the lower abdomen and the perineum (the skin around the anus). Following removal of the cancer, the incision in the perineum is sewn shut. The cut end of the large intestine is attached to an opening in the abdominal wall, called a colostomy. This opening is covered with a bag, which serves to collect stool as it passes through the large intestine and through the colostomy. In contrast to a LAR, the colostomy is permanent.
Many patients would like to avoid a permanent colostomy. When the rectal cancer lies close to the sphincter or anus, an APR is typically recommended. In some instances, a more limited surgery can be used to avoid a colostomy, or radiation therapy can be used to shrink the rectal cancer prior to surgery allowing the patient to maintain control of bowel function. Some small rectal cancers that lie close to the anus can be removed with less extensive surgery called a local excision. Not all patients can undergo a local excision (see Local Excision below).
Patients undergoing an APR may experience lower abdominal pain after the operation. Less common complications related to surgery include bleeding, infection, slow wound healing and temporary difficulty with emptying the bladder. Some men may experience sexual dysfunction after surgery. In-hospital death occurs after APR in less than 5% of patients. Patients should ask the surgeon to explain the various surgical complications and their frequency of occurrence at the hospital where the surgery will be performed.
Sphincter-Sparing Treatment
The rectal sphincter is the circular muscle that controls defecation. If damaged, patients lose control of bowel function. Sphincter-sparing treatment refers to cancer therapy that avoids removal of the anal sphincter for rectal cancers that lie close to the anus. The standard surgical procedure used to remove rectal cancer that lies close to the anus is an abdominoperineal resection (APR). Following an APR procedure, the anus is removed with the cancer, and the cut end of the large bowel is attached to the abdominal wall to form a colostomy. The colostomy is covered by a bag, which collects stool as it empties from the bowel. Because of the inconvenience of a colostomy, physicians are using sphincter-sparing treatments that allow the patient to preserve function of the anus. Sphincter-sparing treatment for rectal cancer involves limited surgery, often followed by a combination of chemotherapy and radiation therapy. The limited surgery is designed to remove the cancer and a small rim of normal bowel, but not the anus. The surgery may be performed through the anus (transanal excision) or through the coccyx (transcoccygeal) or the tailbone. A transanal excision can be performed for small cancers that lie close (within 2 inches) to the anus. Other small cancers higher in the rectum can be removed with a transcoccygeal excision.
Local Excision
Limited surgery can be performed to remove the cancer and preserve the anus and prevent the complications that may occur with more extensive LAR or APR surgeries. The limited surgery is designed to remove the cancer and a small rim of normal bowel, but not the anus. The surgery may be performed through the anus (transanal excision) or through the coccyx (transcoccygeal) or the tailbone. A transanal excision can be performed for small cancers that lie close (typically within 2 inches) to the anus. Other small cancers higher in the rectum can be removed with a transcoccygeal excision.
For limited surgery to be effective, the entire cancer with a rim of normal tissue must be removed. Patients with cancers that are larger, more deeply invading, or appear aggressive under the microscope are better treated with traditional surgery. In order to improve the cure rates after limited surgery alone, a combination of chemotherapy and radiation therapy is often administered for cancers that have grown into the muscular wall of the rectum.
Patients undergoing limited surgery may experience pain in the region of the perineum or tailbone. Less common complications related to surgery include bleeding, infection, and difficulty with healing of the rectal wall. In-hospital fatality is very rare after limited surgery.
Strategies to Improve Treatment
The progress that has been made in the treatment of rectal cancer has resulted from improved surgical techniques and the development of neoadjuvant and adjuvant treatments in patients with more advanced stages of cancer and participation in clinical trials. Future progress in the treatment of rectal cancer will result from continued participation in appropriate clinical trials.
Improved Sphincter-Sparing Treatments: Because of the inconvenience of a colostomy, physicians are using sphincter-sparing treatments that allow patients with low-lying rectal cancers to keep the anus. Improved methods to select patients who can be treated with limited surgery followed by adjuvant chemotherapy and radiation therapy are being developed. More aggressive use of preoperative (neoadjuvant) chemoradiation may allow more patients with larger low-lying rectal cancers a chance to maintain anal function.
Neoadjuvant Therapy: When rectal cancer cannot be completely removed with surgery, a patient’s chance of cure is greatly diminished. Presurgery radiation and/or chemotherapy is referred to as neoadjuvant therapy. Neoadjuvant therapy can shrink some rectal cancers and therefore allow complete surgical removal. Determining the optimal neoadjuvant chemotherapy and radiation therapy is an area of current research.